
Quiz Summary
0 of 40 Questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading…
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 40 Questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
Categories
- Not categorized 0%
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
- 22
- 23
- 24
- 25
- 26
- 27
- 28
- 29
- 30
- 31
- 32
- 33
- 34
- 35
- 36
- 37
- 38
- 39
- 40
- Current
- Review
- Answered
- Correct
- Incorrect
-
Question 1 of 40
1. Question
A 42-year-old previously healthy woman comes to the office due to fever and sore throat. She has no cough. Physical examination shows tonsillar exudate and a nontender cervical lymph node that measures 3.5 cm in diameter. Oral antibiotic therapy is started and on a follow-up visit a week later, the patient reports that her symptoms have resolved. The previously enlarged cervical lymph node has decreased slightly in size. On several follow-up visits over the following year, the patient remains asymptomatic and the size of the lymph node fluctuates but does not disappear completely. Referral to a surgeon is made and excisional biopsy of the lymph node is performed. Which of the following is the most likely diagnosis?
CorrectIncorrect -
Question 2 of 40
2. Question
A 67-year-old man comes to the office after he noticed several nodules in his left axilla. He has a history of malignant melanoma on his upper back, which was treated with wide surgical excision 4 years ago. The patient undergoes biopsy of an axillary lesion, and histopathology reveals melanoma recurrence. Subsequent whole-body positron emission scan shows diffuse metastatic disease involving the lungs, liver, and left axillary nodes. Checkpoint inhibitor therapy with pembrolizumab is initiated, which leads to significant reduction in the size of the axillary nodules and metastatic lesions. Which of the following best correlates with the treatment response in this patient?
CorrectIncorrect -
Question 3 of 40
3. Question
A 45-year-old male returns to clinic for follow-up examination. He has no current complaints and has been feeling well recently. Past medical history is significant for hypertension and gastroesophageal reflux disease. He also had a left knee operation eight months ago that was complicated by a postoperative deep vein thrombosis (DVT) of the left leg. He has no other personal history of blood clots, and there is no family history of clotting disorders. Currently, his vital signs are stable and his physical examination is within normal limits. Specifically, there is no swelling or calf tenderness of the left leg. He took warfarin on a daily basis for a total of six months after the DVT was diagnosed and then stopped taking it because he no longer wanted to deal with monitoring his INR. This is his first visit to clinic since being discharged after his knee operation. Which of the following is the next best step in treating this patient’s prior DVT?
CorrectIncorrect -
Question 4 of 40
4. Question
A 60-year-old woman comes to the emergency department with a daylong history of hematemesis and hypotension. A month ago, the patient was hospitalized for acute pulmonary embolism and underwent anticoagulation with rivaroxaban. In the emergency department, her condition is stabilized after resuscitation with 5 units of packed red blood cells and fresh frozen plasma. Rivaroxaban is discontinued and intravenous proton pump inhibitor therapy is started. Endoscopy reveals a fungating, ulcerated gastric mass suspicious for carcinoma. Because of the major bleeding, inferior vena cava (IVC) filter placement is discussed with the patient. Which of the following considerations is most important to include in the risk-benefit discussion regarding long-term use of the IVC filter?
CorrectIncorrect -
Question 5 of 40
5. Question
A 58-year-old man is brought to the emergency department 30 minutes after a generalized tonic-clonic seizure. His wife witnessed the event and says the patient was watching television, suddenly developed twitching of the left hand, and then lost consciousness and had generalized shaking. The event lasted approximately 1 minute. He spontaneously regained consciousness but has been confused. The patient has no history of seizure, head trauma, or other medical problems, but over the past few months he has had a persistent cough, anorexia, and fatigue and has lost 10 kg (22 lb). He has not seen a physician in 20 years and takes no medications. The patient is a current smoker with a 30-pack-year history and drinks alcohol occasionally. Temperature is 37.2 C (99 F), blood pressure is 138/86 mm Hg, and pulse is 94/min and regular. The patient is somnolent but easily arousable. Bilateral pupils are equal and briskly reactive to light. There is no focal weakness, and deep tendon reflexes are 2+ throughout. Digital clubbing is present and there are several right-sided, enlarged, nonmobile supraclavicular lymph nodes. Blood cell counts and serum chemistry studies are within normal limits, except for a serum calcium level of 10.6 mg/dL. MRI of the brain reveals a 1-cm mass in the gray-white junction of the right frontal lobe with mild surrounding edema. Imaging of the chest and abdomen reveals a 6-cm right lung mass, multiple enlarged hilar and mediastinal lymph nodes, and several liver lesions of 1-3 cm. Which of the following is the most appropriate next step in establishing the diagnosis in this patient?
CorrectIncorrect -
Question 6 of 40
6. Question
A 25-year-old Caucasian man comes to see you in the office because of persistent “lumps” in the neck. He recalls an episode of marked fatigue, fever, pharyngitis, and generalized lymphadenopathy about 8-10 weeks ago, when he was diagnosed with infectious mononucleosis. Most of his symptoms except the neck “lumps” resolved completely in two weeks. On physical examination, he has three anterior cervical lymph nodes, the largest being 2 cm × 2 cm in size. They are mobile and have a firm rubbery consistency. The patient denies any associated symptoms, and the rest of his physical examination is unremarkable. Which of the following is the most appropriate next step in the management of this patient?
CorrectIncorrect -
Question 7 of 40
7. Question
The following vignette applies to the next 2 items
A 56-year-old Caucasian male presents to your office for a routine check-up. He complains of chronic cough, fatigue, and occasional headaches. He has longstanding hypertension, which is controlled with amlodipine and lisinopril. Three months ago, he was diagnosed with acute bronchitis and treated with a short course of antibiotics. He smokes one pack of cigarettes daily and consumes alcohol occasionally. He denies any recreational drug use. His family history is significant for prostate cancer in his father and renal cell carcinoma in his uncle. His blood pressure is 147/82 mmHg, pulse is 93/min, temperature is 36.7 C (98 F), and respirations are 14/min. His oxygen saturation is 94% on room air. His BMI is 42 kg/m2. Physical examination is unremarkable. His chest X-ray is normal.
Hemoglobin 19.2 g/dL Hematocrit 56% MCV 90 fl Reticulocytes 1.5% Platelets 220,000/mm3 Leukocyte count 5,200/mm3 Neutrophils 58% Eosinophils 2% Lymphocytes 33% Monocytes 7% AST 32 U/L ALT 28 U/L Alkaline phosphatase 112 U/L Glucose 102 mg/dL Creatinine 1.0 mg/dL Item 1 of 2
Which of the following is the best next step in managing this patient?
CorrectIncorrect -
Question 8 of 40
8. Question
Item 2 of 2
In three months, his repeat hemoglobin level is 19.0 g/dL. His oxygen saturation in the office is 95% on room air. His carboxyhemoglobin level is normal and serum erythropoietin level is elevated. Iron studies and serum folate and vitamin B12 levels are all normal. Urinalysis shows no blood, no RBCs, and trace protein. Which of the following is the best next step in managing this patient?
CorrectIncorrect -
Question 9 of 40
9. Question
A 65-year-old man comes to the office due to several months of severe fatigue that limits his ability to do daily activities. He has also had upper abdominal fullness, early satiety, and unintentional weight loss but no fever, night sweats, cough, or rash. The patient has not seen a physician for many years. He does not use tobacco, alcohol, or illicit drugs and is a retired chemical engineer. Physical examination shows mucosal pallor with no scleral icterus. The lungs are clear on auscultation, and heart sounds are normal. There is mild hepatomegaly, and the spleen tip is palpable close to the midline of the abdomen. Laboratory evaluation reveals pancytopenia. Peripheral blood smear shows immature granulocytes, nucleated erythrocytes, and teardrop cells. Bone marrow aspiration is attempted but yields no marrow. Which of the following histopathological features is most likely to be present in this patient’s spleen?
CorrectIncorrect -
Question 10 of 40
10. Question
The following vignette applies to the next 2 items
A 52-year-old Caucasian woman comes to the office for a routine follow-up visit. She complains of weakness and fatigue for the past two weeks. She ‘feels tired’ even while doing minor household chores. She denies fever or any changes in appetite or weight. Three months ago, she underwent surgery for carcinoma of the breast and has been on chemotherapy ever since. She is a retired nurse and lives at home with her husband. She was diagnosed with hypertension twenty years ago. Her current therapy includes cyclophosphamide, methotrexate, 5-flurouracil, ondansetron, atenolol and famotidine. Her vital signs are within normal limits. Examination is unremarkable, except for moderate pallor. Rectal examination shows no abnormalities. Her lab results reveal the following:
CBC
Hb
8.5g/dL
MCV
112 fl
Platelet count
100,000/cmm
Leukocyte count
3,500/cmm
Segmented neutrophils
68%
Lymphocytes
26%
Monocytes
6%
Serum chemistry
Serum Na
135 mEq/L
Serum K
3.4 mEq/L
Chloride
106 mEq/L
Bicarbonate
20 mEq/L
BUN
16 mg/dL
Serum creatinine
1.0 mg/dL
Calcium
9.0 mg/dL
Blood Glucose
118 mg/dL
Item 1 of 2
The stool test for occult blood is negative. Which of the following is most likely responsible for her condition?
CorrectIncorrect -
Question 11 of 40
11. Question
Item 2 of 2
Which of the following is the most appropriate pharmacotherapy for this patient?
CorrectIncorrect -
Question 12 of 40
12. Question
The following vignette applies to the next 3 items. The items in the set must be answered in sequential order. Once you click Proceed to Next Item, you will not be able to add or change an answer.
A 62-year-old hospitalized man is evaluated for new-onset, right lower extremity pain. The patient underwent bypass surgery for 3-vessel coronary artery disease 2 months ago. He arrived at the emergency department 2 nights ago due to recurrent chest pains. At that time, ECG showed sinus rhythm with no ST-segment changes, but cardiac troponin I levels were elevated. The patient was initiated on unfractionated heparin, antiplatelet agents, a beta blocker, and a nitrate. A coronary angiogram was performed via the radial artery; it revealed graft insertion site stenosis and was treated with stenting. Postintervention echocardiography revealed left ventricular ejection fraction of 50% with no regional wall motion abnormalities. This morning, the patient had new, sudden-onset, right lower extremity pain. He has never had pain in that extremity before. The patient has a history of hypertension, hyperlipidemia, and type 2 diabetes mellitus. Current medications include aspirin, clopidogrel, rosuvastatin, metoprolol, losartan, isosorbide mononitrate, basal-bolus insulins, and subcutaneous heparin at a prophylactic dose. The patient is a former smoker with a 30-pack-year history. Temperature is 37.6 C (99.7 F), blood pressure is 138/84 mm Hg, pulse is 96/min, and respirations are 18/min. Physical examination reveals normal jugular venous pressure, clear lungs, no heart murmurs, and a soft, nontender abdomen. The right leg is tender and cool to the touch when compared to the left leg. Right lower extremity distal pulses are diminished, but capillary refill is intact. Left leg examination is normal with the exception of healed scars from previous saphenous vein harvesting. Neurological examination is normal. Laboratory results are as follows:
Today
2 days ago
Hemoglobin
12.6 g/dL
13 g/dL
Platelets
77,000/mm3
240,000/mm3
Leukocytes
11,000/mm3
8,200/mm3
INR
1.0
1.1
Serum creatinine
1.0
0.9
Item 1 of 3
Which of the following is the most likely cause of this patient’s leg pain?
CorrectIncorrect -
Question 13 of 40
13. Question
Item 2 of 3
Analgesics and other supportive measures are provided, and vascular surgery is consulted. Diagnostic studies are performed, but the results are pending. Which of the following is the most appropriate next step in management of this patient?
CorrectIncorrect -
Question 14 of 40
14. Question
Item 3 of 3
Immunoassay for heparin-induced thrombocytopenia antibody returns positive. His condition improves with treatment. Which of the following is the most accurate statement regarding heparin use and risk of recurrence of this patient’s current condition?
CorrectIncorrect -
Question 15 of 40
15. Question
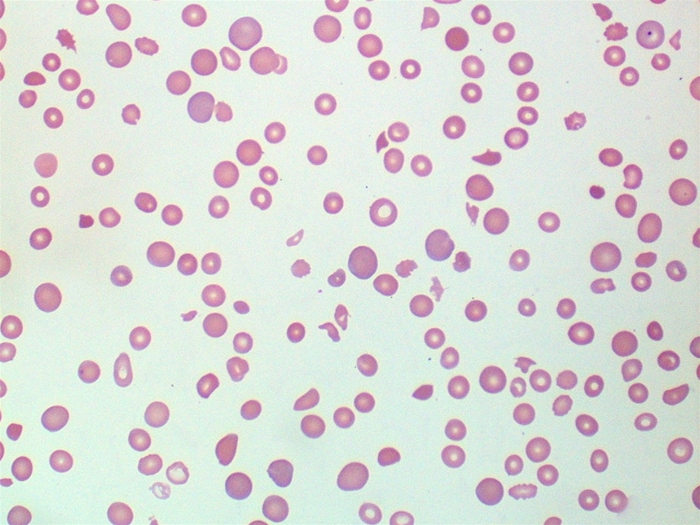
A 45-year-old woman comes to the emergency department due to worsening fatigue. Today, the patient was so tired that she became short of breath doing household chores. She has also had “spots” on her extremities and seems to bruise easily. The patient has had no fever, night sweats, cough, chest pain, palpitations, or abdominal pain. She has no chronic medical conditions and has had no recent cold or flu symptoms. The patient takes no medications and does not use tobacco, alcohol, or recreational drugs. Temperature is 38 C (100.4 F), blood pressure is 110/60 mm Hg, pulse is 92/min, and respirations are 16/min. Physical examination shows moist mucous membranes, clear lung fields, and normal heart sounds. The abdomen is soft and nontender with no hepatosplenomegaly. Neurologic examination is within normal limits. The extremities have no edema, but there are scattered petechiae and ecchymoses bilaterally. Laboratory results are as follows:
Complete blood count
Hemoglobin
8.2 g/dL
Mean corpuscular volume
98 μm3
Platelets
25,000/mm3
Leukocytes
8,000/mm3
Coagulation studies
INR
1.1
Activated PTT
23 sec
Liver function studies
Total bilirubin
2.3 mg/dL
Direct bilirubin
0.7 mg/dL
Aspartate aminotransferase (SGOT)
65 U/L
Alanine aminotransferase (SGPT)
24 U/L
Lactate dehydrogenase
410 U/L
Chest x-ray is normal. A peripheral blood smear is shown in the exhibit. First-line therapy for this patient’s condition exerts its effect through which of the following mechanisms?
 CorrectIncorrect
CorrectIncorrect -
Question 16 of 40
16. Question
A 32-year-old woman comes to the office due to several days of fatigue and malaise. She has no significant medical history and has had no recent sick contacts. The patient does not appear to be in acute distress. Evaluation reveals severe thrombocytopenia. Thrombotic thrombocytopenic purpura is suspected. Which of the following findings is required to make the diagnosis?
CorrectIncorrect -
Question 17 of 40
17. Question
A 36-year-old Caucasian female is seen in the emergency department (ED) for the evaluation of a sudden onset, left lower chest pain and difficulty in breathing. Approximately one year ago, she was diagnosed with left lower extremity deep vein thrombosis secondary to smoking and oral contraceptive pill (OCP) use. At that time, her OCPs were discontinued, she quit smoking, and she was treated with six months of warfarin therapy. She does not have any other medical problems. Her mother and maternal aunt have had “problems with blood clots.” After performing the appropriate ancillary procedures, results reveal the presence of multiple, left-sided pulmonary emboli. A diagnosis of an inherited thrombophilia is suspected. Which of the following is most likely to be present in this patient?
CorrectIncorrect -
Question 18 of 40
18. Question
A 43-year-old male presents to your office with several months history of progressive fatigue and occasional palpitations. He had three episodes of acute respiratory infections over the last year; otherwise, his past medical history is insignificant. He smokes two packs of cigarettes daily and consumes alcohol occasionally. He is not taking any medications and denies drug abuse. He has been sexually active with several partners recently. The physical examination is insignificant. His laboratory values are:
Hb
6.7 g/dL
Red blood cells
2.3 million/cmm
White blood cells
5,900/cmm
Segmented neutrophils
60%
Bands
3%
Eosinophils
2%
Lymphocytes
30%
Monocytes
5%
MCHC
33%
MCV
85 fL
His HIV test results are negative. Which of the following is the best next step in the management of this patient?
CorrectIncorrect -
Question 19 of 40
19. Question
A 1-year-old child is diagnosed with severe microcytic/hypochromic anemia. His past medical history is insignificant. His family history is significant for an early death of his uncle from ‘a blood disease’. Physical examination reveals hepatomegaly and splenomegaly. Subicteric discoloration of the sclerae is present. If this child survives several years after the diagnosis, severe organ damage due to iron overload is best explained by which of the following?
CorrectIncorrect -
Question 20 of 40
20. Question
A 57-year-old woman comes to the primary care physician for a follow-up visit after undergoing a screening colonoscopy. The colonoscopy revealed adenocarcinoma of the ascending colon and 2 well-differentiated, sessile, adenomatous polyps of the sigmoid colon. The patient has a history of mitral valve prolapse and fibromyalgia. She has also had a prior hysterectomy. Her medications include hormone replacement therapy and ibuprofen. The patient eats a high-fiber vegetarian diet and has consumed 3-4 alcoholic beverages per day for the past 30 years. She smoked 1 pack of cigarettes a day for nearly 5 years, but quit 30 years ago. There is no family history of cancer. The patient is very concerned about being diagnosed with colon cancer. Which of the following was her most significant risk factor for developing colon cancer?
CorrectIncorrect -
Question 21 of 40
21. Question
The following vignette applies to the next 3 items.
A 70-year-old woman comes to the office due to back pain, fatigue, and inability to carry out her daily work. The pain began 6 months ago and has slowly intensified. The patient had a hip fracture 3 months ago but has no other medical conditions. She is a lifetime nonsmoker and drinks alcohol on social occasions. She currently takes no medications. The patient has no extremity weakness or paresthesia. She has mild constipation; urination is normal. Initial laboratory results are as follows:
Complete blood count
Hemoglobin
12 g/dL
Mean corpuscular volume
85 µm3
Platelets
220,000/mm3
Leukocytes
4,500/mm3
Neutrophils
56%
Eosinophils
1%
Lymphocytes
33%
Monocytes
10%
Serum chemistry
Creatinine
2.1 mg/dL
Calcium
11.6 mg/dL
Total protein
8.5 g/dL
Erythrocyte sedimentation rate
75 mm/h
Dipstick urinalysis is normal.
Item 1 of 3
Which of the following is the best next step in management of this patient?
CorrectIncorrect -
Question 22 of 40
22. Question
Item 2 of 3
The patient undergoes a bone marrow biopsy, which shows 20% plasma cells. While discussing the options for further investigation and treatment, the patient says that, since her initial visit, she has had pain in her left shoulder and right flank after a minor fall. Which of the following is the best next step in management?
CorrectIncorrect -
Question 23 of 40
23. Question
Item 3 of 3
The patient is informed about the prognosis, potential risks, and benefits of therapy. She declines treatment. The physician documents their discussions and arranges for follow-up visits. One month later, the patient is brought to the emergency department by family members due to acute-onset blurry vision, headache, confusion, and epistaxis. A detailed history from the family members fails to identify any precipitating factor. On examination, the patient is lethargic but arousable. Scant gingival bleeding is noted. The lungs are clear to auscultation; there is no peripheral edema. Serum creatinine is 2.4 mg/dL. Which of the following is the most likely cause of this patient’s acute change in status?
CorrectIncorrect -
Question 24 of 40
24. Question
A 58-year-old Caucasian man comes to the office with complaints of cough for the past two months and blood-tinged sputum for the past three days. He has lost approximately 25 pounds over the past six months. He denies any history of low-grade fevers or night sweats. He has a long history of heavy smoking and chronic obstructive pulmonary disease. His temperature is 37.0C (99F), blood pressure is 120/62 mmHg, and heart rate is 82/min. He is a thin, cachectic man who is in no acute distress. Lung auscultation reveals the presence of rales in the right upper lung fields. His white cell count is 8,000/cubic mm with normal differential count. His serum calcium level is 12.8 mg/dL. His chest x-rays shows a 3.2 cm mass in the right upper lung zone, which is suspicious for a lung malignancy. Sputum cytology reveals poorly differentiated squamous cell carcinoma. Pulmonary function testing shows that his FEV1 is 1200 cc, while quantitative ventilation-perfusion scan shows that 65% of his pulmonary function comes from his right lung. What is the next best step in the management of this patient?
CorrectIncorrect -
Question 25 of 40
25. Question
A 60-year-old man has experienced progressive shortness of breath over the last 6 months that is occasionally accompanied by chest pain. He was diagnosed with hypertension 10 years ago. Twenty years ago, he suffered from advanced-stage Hodgkin lymphoma that was treated with combination chemotherapy and radiation therapy. He is a lifetime nonsmoker. Blood pressure is 138/90 mm Hg and pulse is 78/min and regular. Physical examination shows a 2/4 early diastolic murmur at the left sternal border. Echocardiogram shows an enlarged left atrium, a normal-size left ventricle with an ejection fraction of 60%, and moderate diastolic dysfunction. Both the mitral and aortic valves appear sclerotic and calcified. The aortic root is normal-size but is echo bright. There is moderate aortic regurgitation. Cardiac catheterization shows ostial narrowing of the right and left main coronary arteries. Which of the following is the most likely diagnosis?
CorrectIncorrect -
Question 26 of 40
26. Question
A 67-year-old woman comes to the emergency department due to sudden, severe low back pain that began after she lifted her grandson. The pain does not radiate to the lower extremities, and the patient has had neither weakness nor sensory loss in her legs nor urinary incontinence. The patient has been feeling tired lately; she has also had a poor appetite and lost 4.5 kg (10 lb) over the past several months. Medical history includes osteoporosis diagnosed on screening DXA at age 65, for which she takes calcium and vitamin D daily and alendronate weekly. The patient is a lifelong nonsmoker and drinks alcohol occasionally. Blood pressure is 148/86 mm Hg and pulse is 96/min. BMI is 21 kg/m2. On physical examination, tenderness to percussion is noted over the lower thoracic spine. Bilateral lower extremity muscle strength, sensation, and deep tendon reflexes are normal. Laboratory results are as follows:
Complete blood count
Hemoglobin
10.4 g/dL
Mean corpuscular volume
92 µm3
Platelets
240,000/mm3
Leukocytes
9,000/mm3
Serum chemistry
Sodium
135 mEq/L
Potassium
3.8 mEq/L
Chloride
106 mEq/L
Bicarbonate
24 mEq/L
Blood urea nitrogen
24 mg/dL
Creatinine
1.1 mg/dL
Calcium
10.6 mg/dL
Glucose
94 mg/dL
Liver function studies
Total protein
8.1 g/dL
Albumin
3.5 g/dL
Total bilirubin
0.8 mg/dL
Alkaline phosphatase
200 U/L
Aspartate aminotransferase (SGOT)
32 U/L
Alanine aminotransferase (SGPT)
24 U/L
Thyroid-stimulating hormone
3.4 µU/mL
Parathyroid hormone
pending
Spine radiography reveals a T12 vertebral compression fracture. In addition to analgesics, which of the following is the most appropriate next step in management of this patient?
CorrectIncorrect -
Question 27 of 40
27. Question
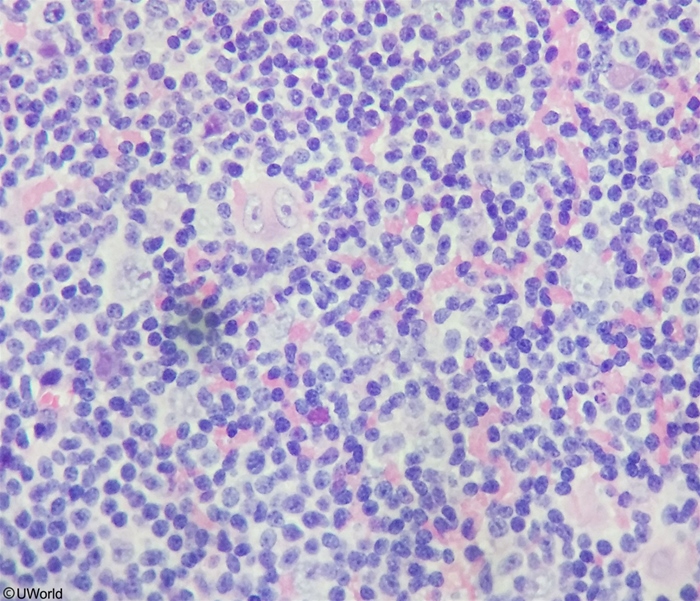
A 60-year-old man comes to the clinic due to 2 months of fatigue. He has also had an intermittent cough and fever, for which he takes ibuprofen. The patient is otherwise healthy and takes no other medications. He does not smoke cigarettes or drink alcohol. Weight is 72.5 kg (160 lb), decreased from 79.4 kg (175 lb) 6 months ago. Temperature is 38 C (100.4 F), and pulse is 110/min. Cervical and axillary lymphadenopathy is present. Cardiopulmonary examination is unremarkable. The liver is palpable 4 cm below the costal margin. Skin examination shows pallor but is otherwise unremarkable. Complete blood count results are as follows:
Hemoglobin
9.5 g/dL
Platelets
160,000/mm3
Leukocytes
13,800/mm3
Neutrophils
60%
Eosinophils
4%
Lymphocytes
32%
Monocytes
4%
Biopsy of a lymph node is shown in the exhibit. Which of the following is the best next step in evaluation of this patient?
 CorrectIncorrect
CorrectIncorrect -
Question 28 of 40
28. Question
The following vignette applies to the next 2 items. The items in the set must be answered in sequential order. Once you click Proceed to Next Item, you will not be able to add or change an answer.
A 72-year-old woman is brought to the emergency department due to worsening generalized weakness. The patient has had fatigue and an unintentional weight loss of 4.5 kg (9.9 lb) over the past month. Outpatient evaluation revealed anemia, splenomegaly, and diffuse lymphadenopathy. Lymph node biopsy and bone marrow aspiration biopsy 2 weeks ago established a diagnosis of high-grade B-cell lymphoma. The patient has not yet started treatment. Over the past 4 days, she has had increasing nausea, poor oral intake, weakness, and lethargy. Medical history also includes hypertension and osteoporosis. Temperature is 36.4 C (97.5 F), blood pressure is 116/68 mm Hg, pulse is 90/min, and respirations are 16/min. BMI is 22 kg/m2. On physical examination, the patient appears frail. Neck veins are flat. Lung sounds are clear, and no cardiac murmurs are present. The abdomen is nondistended, soft, and nontender. Laboratory studies are as follows:
Complete blood count
Hemoglobin
9.6 g/dL
Platelets
240,000/mm3
Leukocytes
7,500/mm3
Serum chemistry
Sodium
130 mEq/L
Potassium
5.1 mEq/L
Bicarbonate
22 mEq/L
Blood urea nitrogen
40 mg/dL
Creatinine
2.1 mg/dL
Calcium
8.0 mg/dL
Phosphorus
5.5 mg/dL
Renal function studies were within normal limits 2 weeks ago. There is no hydronephrosis on renal ultrasonography.
Item 1 of 2
Which of the following is the best next step in evaluation of this patient’s renal dysfunction?
CorrectIncorrect -
Question 29 of 40
29. Question
Item 2 of 2
The serum uric acid level is 13.3 mg/dL. Which of the following is the best next step in management of this patient?CorrectIncorrect -
Question 30 of 40
30. Question
A 67-year-old man comes to the physician with a 3-week history of right shoulder pain. The pain is dull, occurs mostly at night, and is poorly responsive to over-the-counter analgesics. He has had no trauma to his shoulder. His past medical history is significant for hypertension, type 2 diabetes mellitus, and chronic lower back pain. The patient is a lifetime nonsmoker. His last hemoglobin A1c was 8.2%, and prostate-specific antigen checked a few weeks ago was 22 ng/mL (normal <4 ng/mL). On physical examination, the right shoulder has full range of motion and no local tenderness. There is decreased vibration sense at both ankles and first metatarsal heads. Digital rectal examination shows an enlarged nodular prostate. Plain radiographs of the right shoulder show no abnormalities. Results of a transrectal prostate biopsy are pending. Which of the following is the best next step in management of this patient’s shoulder pain?
CorrectIncorrect -
Question 31 of 40
31. Question
A 32-year-old female is seen for a follow-up visit six months after undergoing total thyroidectomy and central neck dissection for medullary thyroid cancer. Pathology results revealed that the tumor was 3 cm in diameter, and 3 of 18 dissected nodes were positive for malignancy. The fasting serum calcitonin level before surgery was 250 ng/ml (normal < 4ng/ml). The postoperative course was uncomplicated, and she was then started on levothyroxine 0.15 mg/d. The repeat TSH level obtained after 8 weeks was normal. The physical examination revealed no abnormal neck masses. The rest of the examination is also unremarkable. Her current calcitonin level is 120 ng/ml. What is the next best step in the management of this patient?
CorrectIncorrect -
Question 32 of 40
32. Question
A 66-year-old woman comes to the office to have a lipoma removed from her elbow. The lipoma does not cause her pain, but she does not like the way it looks when she wears sleeveless dresses. Her other medical problems include hypertension and gastroesophageal reflux. Review of systems is positive for 8 months of general malaise and fatigue, which the patient attributes to having started a more difficult Pilates routine. Temperature is 37.2 C (98.6 F), blood pressure is 108/72 mm Hg, and pulse is 66/min. Physical examination shows mild pallor and mobile, firm lymphadenopathy in her cervical and supraclavicular chains. The jugular veins are not distended. Cardiopulmonary and abdominal examinations are normal. Her preoperative blood count is as follows:
Complete blood count Hemoglobin 10.2 g/dL Platelets 84,000/mm3 Leukocytes 48,800/mm3 Neutrophils 19% Lymphocytes 80% Monocytes 1% Flow cytometry confirms the diagnosis. Which of the following is correct about this patient?
CorrectIncorrect -
Question 33 of 40
33. Question
A 34-year-old woman is admitted with a diagnosis of acute lymphoblastic leukemia (ALL). She is scheduled to receive induction chemotherapy with vincristine, doxorubicin, and prednisone. She has no other past medical history. She has never smoked or used recreational drugs. Which of the following tests is the most appropriate for monitoring this patient’s condition while on chemotherapy?
CorrectIncorrect -
Question 34 of 40
34. Question
A 66-year-old man is evaluated for fatigue and anorexia. Examination shows splenomegaly and inguinal and axillary lymphadenopathy. Excisional lymph node biopsy establishes the diagnosis of diffuse large B-cell lymphoma of germinal center B subtype. Treatment with combination cytotoxic chemotherapy and rituximab is planned. Pretreatment medical evaluation shows normal kidney function, and the patient receives rasburicase with chemotherapy. Four days after treatment, laboratory results are as follows:
Serum chemistry
Sodium
140 mEq/L
Potassium
4.8 mEq/L
Bicarbonate
24 mEq/L
Blood urea nitrogen
36 mg/dL
Creatinine
2.9 mg/dL
Calcium
6.6 mg/dL
Phosphorus
10.4 mg/dL
Uric acid
6.2 mg/dL
Which of the following best explains this patient’s laboratory findings?
CorrectIncorrect -
Question 35 of 40
35. Question
A 55-year-old Caucasian male presents to your office complaining of easy fatigability. He used to be physically active and always preferred to walk to work, which is five blocks away from where he lives. Now he says, “Doc, I get short of breath when I walk even two blocks.” He denies any palpitations, chest pain, cough, or lower extremity swelling. He does not feel down and has no problems with sleep. His past medical history is insignificant. He is currently not taking any medications. His blood pressure is 120/70 mm Hg and heart rate is 95/min. The physical examination is significant for pallor of the conjunctivae and oral mucosa. His laboratory values are:
Hemoglobin
7.2 g/L
Erythrocyte count
3.5 ml/mm3
MCHC
27%
MCV
72 fl
Platelets
200,000/mm3
Leukocyte count
4,500/mm3
Neutrophils
56%
Eosinophils
1%
Lymphocytes
33%
Monocytes
10%
Serum ferritin
24 ng/mL
Blood smear analysis shows microcytic erythrocytes with anisocytosis. What is the best next step in the management of this patient?
CorrectIncorrect -
Question 36 of 40
36. Question
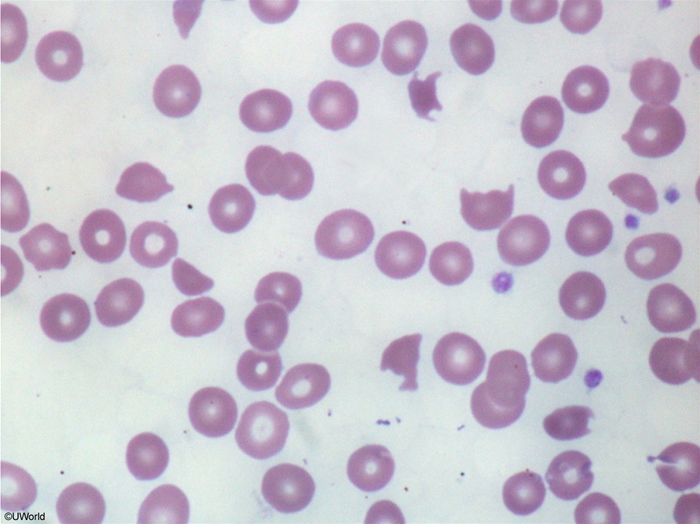
A 29-year-old woman comes to the emergency department due to fever and headache for the last week. The patient has a generalized tonic-clonic seizure while being evaluated. Laboratory results are as follows:
Hemoglobin
6.1 g/dL
Platelets
16,000/mm3
Creatinine
2.2 mg/dL
Total bilirubin
4.3 mg/dL
Serum haptoglobin
undetectable
PT
11 sec (INR 1.1)
Activated PTT
30 sec
Peripheral blood smear is shown in the exhibit. Which of the following is the most likely underlying cause of this patient’s current condition?
 CorrectIncorrect
CorrectIncorrect -
Question 37 of 40
37. Question
The following vignette applies to the next 2 items
A 54-year-old man with new-onset type 2 diabetes mellitus comes to the physician for his first screening ophthalmologic examination. He has no eye symptoms and describes his vision as excellent. He does not smoke. His family history is significant for obesity and diabetes but negative for cancer. Funduscopic examination shows a small, densely pigmented lesion with irregular borders in the peripheral right choroid. The lesion is about 8 mm in diameter and is minimally raised (1 mm). Comprehensive skin examination is unremarkable.
Item 1 of 2
Which of the following should be the next step in the management of this patient?
CorrectIncorrect -
Question 38 of 40
38. Question
Item 2 of 2
The patient is lost to follow-up. He returns 2 years later due to intermittent blurry vision. His HbA1c is 8.2%. Repeat funduscopic examination shows that the pigmented lesion now measures 18 mm in diameter and its height is estimated at 4 mm. Comprehensive skin examination is unremarkable. Further evaluation shows no lesions beyond the right eye. Which of the following is the best next step in the management of this patient?
CorrectIncorrect -
Question 39 of 40
39. Question
The following vignette applies to the next 2 items
A 45-year-old Caucasian female presents to your office with abdominal discomfort and distention that is especially bothersome after meals. She has noticed recently that she gets tired more easily. She feels “down”, but denies any sleep difficulty, crying spells and suicidal ideation. She visited a doctor approximately one year ago due to similar complaints, and was told that the problem was psychological. She underwent myomectomy for a large uterine fibroid 8 years ago. She is not sexually active. Her family history is significant for pancreatic cancer in her father and a thyroid disease in her mother. The physical examination is significant for mild pallor of the conjunctivae. The abdomen is somewhat distended with no palpable masses. The laboratory values are:
Hemoglobin
8.8 g/L
MCV
117 fl
Platelets
200,000/mm3
Leukocyte count
4,500/mm3
Neutrophils
56%
Eosinophils
1%
Lymphocytes
33%
Monocytes
10%
Serum iron
110 mg/dL
Serum cobalamin
90 pg/ml (N > 300 pg/ml)
Serum folate
12.5 ng/ml (N > 4.0 ng/ml)
Item 1 of 2
What is the best next step in the management of this patient?
CorrectIncorrect -
Question 40 of 40
40. Question
Item 2 of 2
After taking the appropriate initial steps, you proceed with gastric endoscopy. Which of the following findings is more likely to be present in this patient?
CorrectIncorrect